Amazing experimental laryngeal masks made by Dr. Archie Brain on his journey from an idea to reality
We will discuss the following aspects. Please scroll down and start reading.
- How the idea of the laryngeal mask first emerged
- Goldman rubber cuffs
- Latex cuffs
- Silicone cuffs
- Trying to increase the seal pressure
- The problem of the epiglottis
- Gastric channel
- Intubation aid
How the idea of the laryngeal mask first emerged
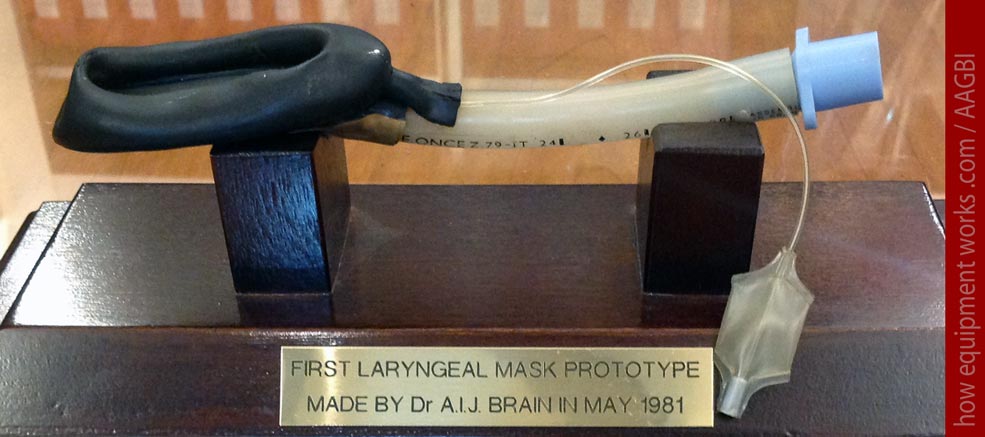
My fascination for the history of the laryngeal mask airway started when I went to a study day at the Association of Anaesthetists in Great Britain and Ireland ( I know it is a tedious long title) located in London. It wasn’t the study day itself that fascinated me. Rather, during the coffee break, I discovered a little museum housed in the building. In this museum holding anaesthesia-related historical items, I saw in a glass case, the device shown below. What was on display was a very early experimental version of the laryngeal mask made in the year 1981. As I looked at it, I was completely amazed by how that crude handmade device is a forerunner of the laryngeal mask, which as an anaesthetist, I have ( and probably you have as well) used so many thousands of times.

At the time I saw this early laryngeal mask in the museum, I didn’t really know much about the history of this device. I have since looked for more information and have discovered that its history is associated with many wonderful experimental designs. In this web page, I hope to share with you a glimpse of this fascinating history using pictures of many of the original experimental versions. After reading this, the next time you insert a laryngeal mask, you will know where it all began. However, to appreciate the historical significance of the laryngeal mask, we need to use a time machine and move back to the early nineteen eighties.
In the early 1980’s, before the laryngeal mask was invented, there were two basic ways of maintaining an airway. One was to use a face mask and the other was to use a tracheal tube. Using a face mask for anything but the shortest anaesthetics was not a reliable way to maintain an airway and it was tedious to hold the mask. One had the possibility of attaching rubber straps to keep the mask in place, but these often didn’t work well. When using the mask with these straps, one had to often concentrate more on managing the airway than managing the rest of the patient and anaesthetic.
The alternate option to using a face mask was to place a tracheal tube. At times, this was needed for a good reason, such as when giving anaesthesia to a patient with a full stomach. But at other times, it was put in because the face mask wasn’t doing its job well. This meant that, if a more reliable mask could be invented, a large number of unnecessary intubations ( and their associated complications) could be avoided.
Now the hero of this story makes an entrance. His name is Dr. Archie Brain and he (aged about 38 at the time) was working as an anaesthetist in the beautiful island country of Seychelles. While working there, he encountered two difficult airways.

The two encounters with difficult airways got him thinking about whether there was a better way of managing patient airways.
Dr Brain returned to the United Kingdom and joined the Royal London Hospital in 1981 as a lecturer. Decades later, I too trained there but never knew that it was connected with the birth of the laryngeal mask. The blue arrow points to where the emergency operation theatres were located. I remember how towards the end of the night shifts, some of us would stare out of the windows to see if we could see the day staff entering the hospital to take over cases from us.
Initially, Dr. Brain was involved in a variety of projects at the Royal London Hospital but was not focused on one direction. Then one day there was a lecture by an American anesthesiologist ( Dr. Lucien Morris) who talked about the problems associated with tracheal tubes and how the future of airway management should take a different direction. Dr. Brain was in the audience listening very carefully.
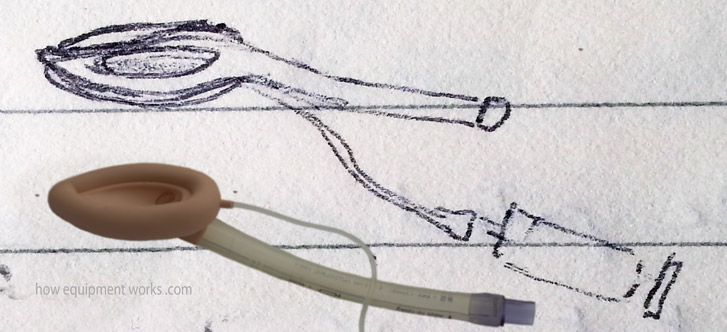
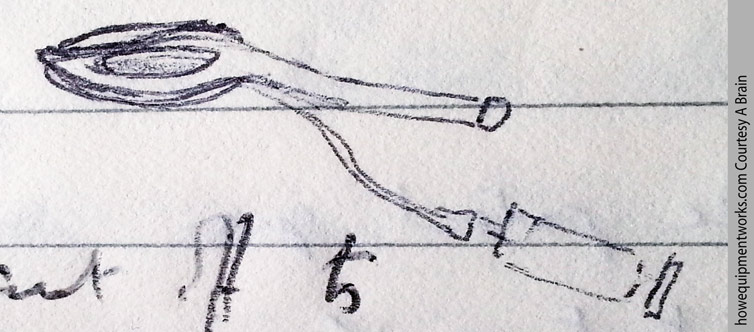
This lecture reminded him about his own quest started in Seychelles, to find an alternative airway management method to that existing at that time. He now focused his research at the Royal London Hospital on finding a suitable airway solution. As he kept thinking of various solutions to the problem, Dr. Brain recorded his thoughts in diaries. Shown below is an actual image taken from one of his diaries. It shows a diagram, drawn in 1981, that shows the laryngeal mask concept, that resembles what we use today, for the first time. It is interesting that this early diagram even has a syringe!
Here is an excerpt from the diary around the period when the drawing was made. I have “translated” his handwriting in case you struggle to read it.
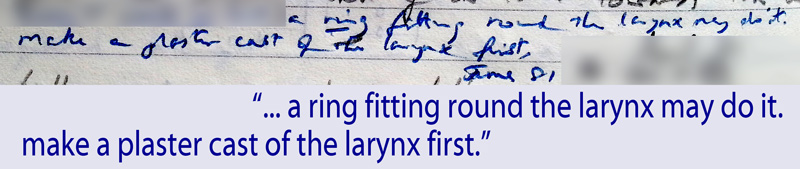
As the above diary entry shows, to better understand the airway, he made plaster casts of actual specimens of the larynx.
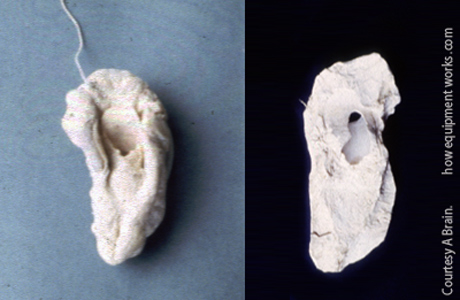
Analysing the casts, he realised that the laryngeal inlet had an oval shape. He wondered if it would be possible to create a seal using such a shape.

Goldman rubber cuffs
The story of the laryngeal mask has a lot of lucky coincidences. One was that, as part of his duties, he had to anaesthetise patients having dental extractions. At that time, dental anaesthesia involved using a very special mask called a “Goldman Nasal Mask”. This mask, which was held over the nose, gave the dental surgeon good access to the mouth.
To facilitate cleaning, this mask had a rubber cuff that could be detached ( nothing was disposable back then !). It was these cuffs that interested Dr. Brain.

Dr Brain noticed that the shape (contour) around the nose seemed to be similar to the shape around the laryngeal inlets that he had been studying.

He then wondered if cuffs taken from Goldman Masks, which were normally used over the nose, could be modified to fit over laryngeal inlets.

Dr Brain decided to make an experimental device to study the concept further. He removed the cuff from the Goldman mask.
The rubber Goldman cuff had a thin strip around it called a flange (shown in light grey below). The flange was used to attach the cuff to the rest of the mask.
Dr. Brain took a tracheal tube and cut it as shown below. The Goldman cuff was taken and the flange (shown in grey) was brought together and glued onto the cut tracheal tube to form a laryngeal mask.
Here is a close-up image of a real Goldman cuff-based experimental laryngeal mask that shows the above method of construction. In the early days of the laryngeal mask, Dr. Brain struggled to get it commercially produced. He even tried to get them made by hand in the Seychelles and the example below was made by one of the “trainee” workers there. This explains why the glueing is not perfect.
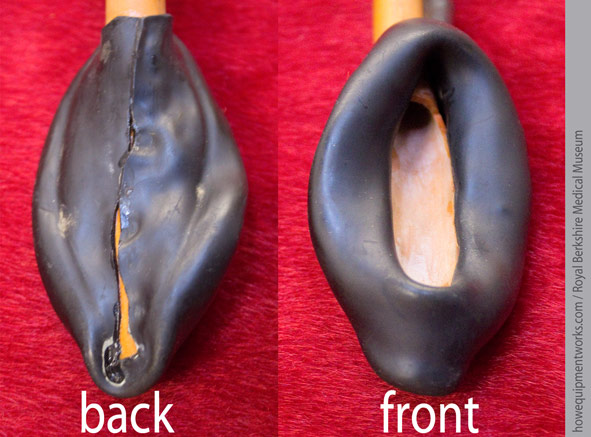
Here is the full view of the above mask.

Here is a version made by Dr. Brain himself.
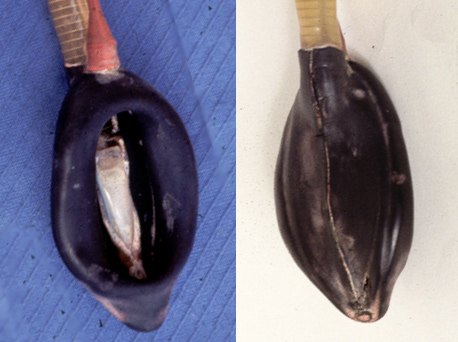
And this is the Goldman cuff laryngeal mask that I first saw in the museum.
Dr. Brain kept these experimental versions in his car and took them wherever he went. They remained like this for six weeks, till one day in August 1981, for the first time in the world, one was inserted into a patient. The patient happily breathed through the laryngeal mask and Dr. Brain gently squeezed the breathing system bag and found that it also worked well providing positive pressure ventilation.

Do you work in the anaesthetic team? If you do, please visit the free website below, which has anaesthesia-related fun and safety material. Click the button below to visit.

While the first laryngeal mask use was a complete success, for Dr. Brain and the laryngeal mask, the long journey ahead had only begun. There were huge challenges ahead.
Dr. Brain made a few more experimental laryngeal masks and after getting ethics approval, did a pilot study. There is a lesson here for those of us who lose hope when our submissions to journals are rejected. Dr. Brain’s first submission of this landmark paper was rejected by the journal! Considering that there are now many thousands of journal articles on laryngeal masks, it is almost unimaginable that the first one was nearly not published!
In the first four years of Dr. Brain’s work on the laryngeal mask, he made about 70 experimental laryngeal masks using Goldman cuffs!
Inserting it into himself!
Very early on, Dr Brain was convinced that the laryngeal mask was gentle to the airway and decided to demonstrate it to himself. In February 1983, he went to the photography department at the Royal London Hospital and asked them to take pictures of him inserting a laryngeal mask into his own pharynx. Dr. Brain sprayed his oral cavity with lignocaine and self-inserted it four times. Just imagine what went through the photographer’s mind when Dr. Brain popped it into his mouth! The image below shows Dr. Brain looking at the laryngeal mask during that photo session.
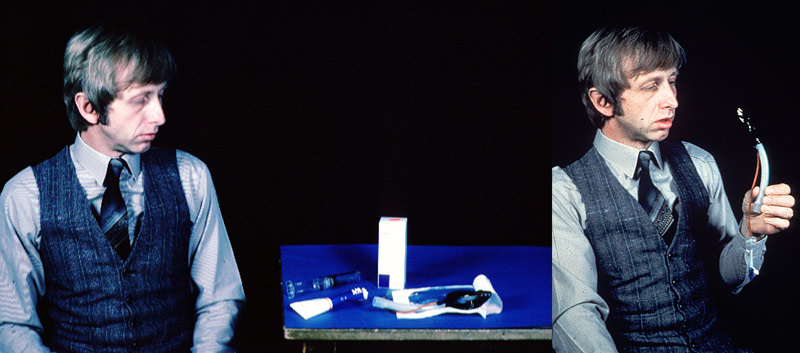
Unfortunately, the original image of the laryngeal mask actually inside his mouth was lost during one of Dr. Brain’s lectures ( this was at a time when there was no PowerPoint and laptops). I have therefore, using the first two images, reconstructed a third image showing him with the laryngeal mask in his mouth ( scary isn’t it, what computer image manipulation can do !).

At this point, let me tell you how I managed to contact Dr. Brain to help me with information for this website. Dr. Brain was living a peaceful life till I got interested in the early experimental laryngeal masks. The quest to find more information started with my brother-in-law, Esala Weerakoon ( see photo below). He is a diplomat and was travelling to a place near where Dr. Brain was staying. I asked him if he could try and meet Dr Brain …. and thankfully he agreed.

I gave my brother-in-law a letter to hand deliver to Dr. Brain, just in case he was able to meet him. Below are some actual sentences taken from the letter.
Fortunately, Dr. Brain did not throw the letter into the dustbin! In fact, he has done exactly the opposite. He has been extremely helpful, spending huge amounts of time answering my queries. I was also really fortunate to ultimately meet the great man himself.

Let us now return to laryngeal masks.
Latex cuffs
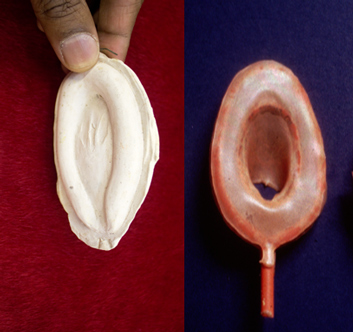
After about four years since starting work on the laryngeal mask, the Goldman cuffs were no longer produced and were hard to come by (maybe Dr Brain used up all that was left !). Furthermore, the Goldman cuffs were available only in one size and were difficult to make into different shapes. Dr Brain decided to make his own cuffs using liquid latex ( a form of rubber). This involved hard work as he had to do it all by himself. I will briefly describe the process. First Dr. Brain would make a mould using Plaster of Paris. These were based on information he got from cadaver studies.
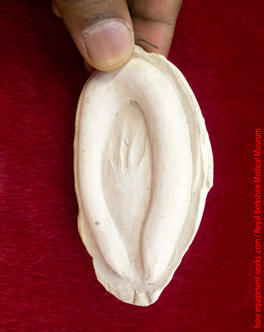
This mould would be dipped in liquid latex and removed. Once the latex that clung onto the mould dried, it would be peeled off to form a cuff. The process took many hours and there were many failures.
Here is an actual mould and latex cuff.
The curvature of the bowl of the laryngeal mask ( pink area ) is an important part of laryngeal mask design. Dr. Brain needed to find a way to make this bowl.
Dr. Brain, as usual, made use of things available around him. To create the bowl shape, he used ordinary teaspoons! The image below shows a straight-ended tube (1) that needs to have a bowl-shaped curvature at the end, which would eventually be attached to the cuff ( 2 ). Dr. Brain would put the end of the plastic tube between two spoons which were then heated to make the end soft ( 3, 4 ).
The tube would then be left to cool and harden ( 1 ). When the spoons were removed ( 2 ), there would be a nice bowl shape to attach to the cuff ( 3 ).
Here is one of the original spoons Dr. Brain used.

Please click the “Next” button below to read part 2 of our discussion on amazing experimental laryngeal mask airways. Thank you.