Note: This is part 2 of the discussion of tracheal tubes. If you have not read part 1, please click here to go to part 1.
PEDIATRIC endotracheal tubes
Endotracheal tubes for paediatric patients are smaller than those meant for adults. Because the paediatric trachea is susceptible to damage by pressure, most paediatric endotracheal tubes are uncuffed. However, cuffed versions similar to adult endotracheal tubes exist and when used, must be inflated with care. A wide range of sizes are available.
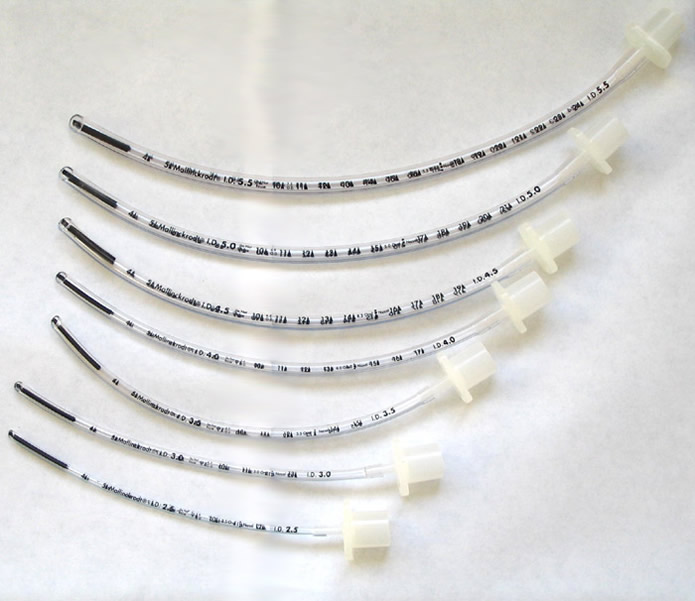
Formulae are available to guide size selection. After intubation, depending if the fit is too tight or loose, one may have to use a different size of endotracheal tube. For this reason, one should always keep a wide range of paediatric endotracheal tube sizes.
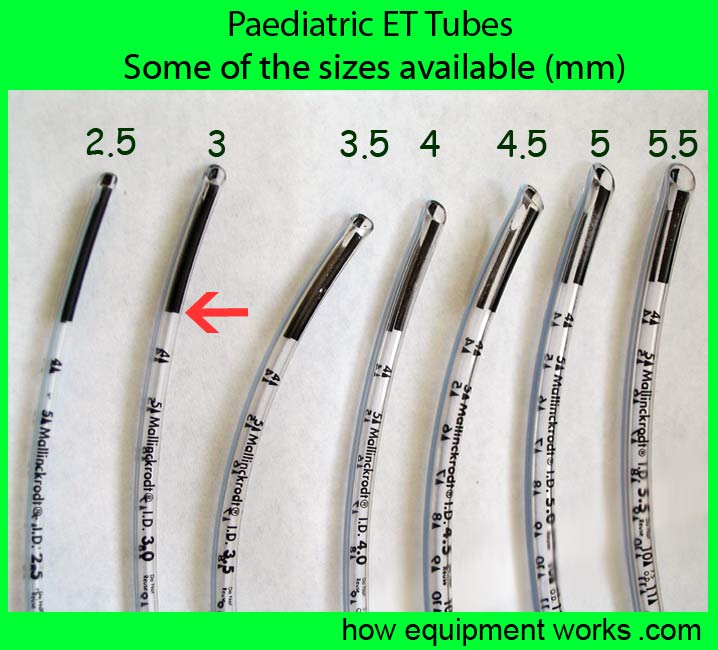
The endotracheal tubes may have a mark to guide the optimum depth of placement. In these endotracheal tubes, the vocal cords should be at the junction (see red arrow) between the black area and clear area as shown below.
Reinforced / armoured endotracheal tubes
Reinforced or armoured endotracheal tubes are specially designed to be resistant to kinking.
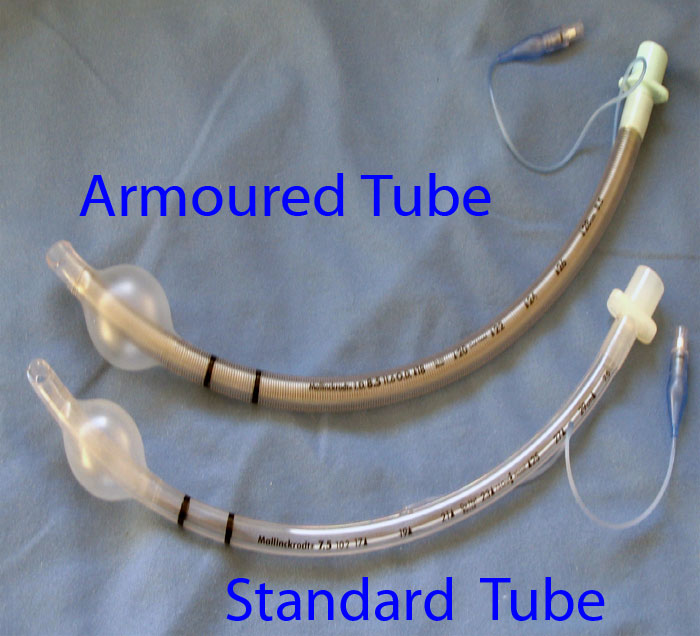
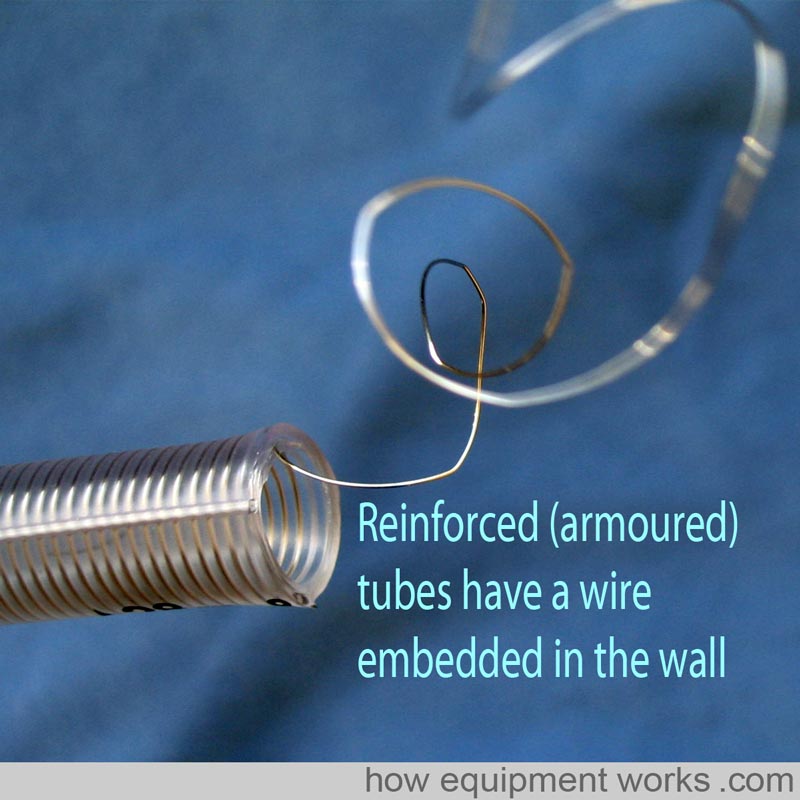
As shown below, they achieve this property by having a spiral of wire embedded into the wall of the endotracheal tube to give it strength and flexibility at the same time. These are particularly useful for head and neck surgery where the endotracheal tube may be sharply bent and also compressed by the surgeons. Armoured endotracheal tubes can be easily bent away from the area of surgery and thus improve surgical access.
LASER RESISTANT endotracheal tubes
Some airway surgery involves the use of laser beams to burn away tissue. These beams can ignite ordinary endotracheal tubes and in the presence of Oxygen may cause major airway fires. Special endotracheal tubes are available (example shown below) which resist damage by laser beams.
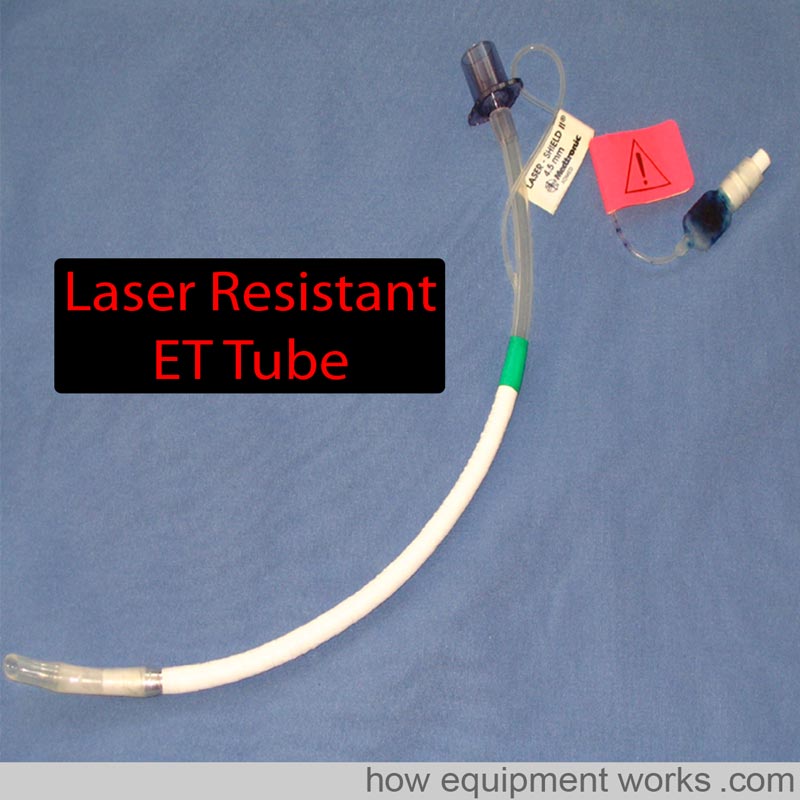

In the endotracheal tube shown, there is a laser-resistant metal foil wrapped around it for protection.

The cuff of laser-resistant endotracheal tubes is usually filled with saline instead of air to minimise the risk of fire. The saline may be coloured blue using methylene blue dye. As will be shown to you in the next picture, this helps to detect cuff rupture due to fire.

If the laser manages to damage the cuff, the colouring will help identify rupture and the saline will help prevent an airway fire.


Do you work in the anaesthetic team? If you do, please visit the free website below, which has anaesthesia-related fun and safety material. Click the button below to visit.

Double lumen tubes
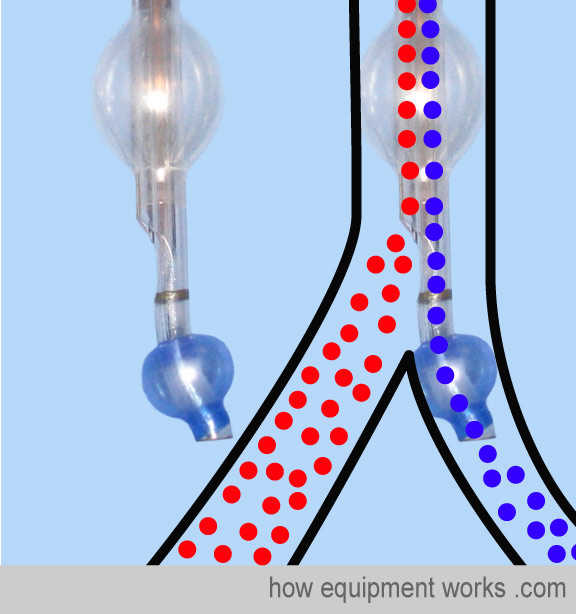
In thoracic surgery, there are times that you may need to isolate and selectively not ventilate one lung. For example, during an oesophagectomy, one may choose to not ventilate one lung to provide better surgical access to the oesophagus. There are special endotracheal tubes called “double lumen tubes “ to achieve this. A double-lumen tube can be thought of as two endotracheal tubes joined together (see graphic below). One tube is shorter and ends in the trachea and there is a cuff at this level called the tracheal cuff (coloured red in the image). The other tube extends further and enters one of the main bronchus and has its own cuff (bronchial cuff, usually coloured blue).
Using a special connector and clamp, one can avoid ventilating one lung and let it collapse to provide good surgical access.
Here are some close-up images of actual double-lumen tubes.
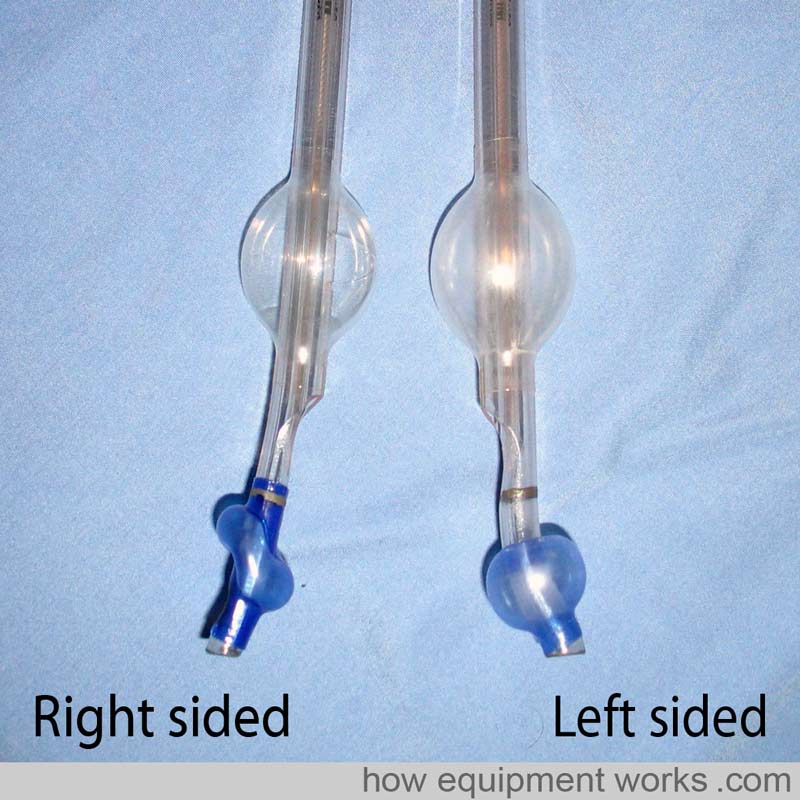
The image shows a left-sided double-lumen tube. The bronchial end (blue cuff) is inside the left bronchus.
Bronchial blocker
An alternative to using a double-lumen tube to isolate one lung is to use a standard endotracheal tube along with a special device called a “bronchial blocker”. The bronchial blocker has a thin tube with a cuff at one end.
Let us isolate the left lung using a bronchial blocker. First, the trachea is intubated with a standard endotracheal tube. As expected, you will be now ventilating the left lung and the right lung.
The bronchial blocker is inserted through the standard endotracheal tube you just inserted. It is guided into the left lung, often using a fibre optic scope.
Once positioned correctly, the cuff of the bronchial blocker is inflated. This cuff blocks air entry into the left lung. The air in the left lung escapes through the thin bronchial blocker tube (shown in pink ) making the left lung collapse. Ventilation to the right lung continues through the standard endotracheal tube (shown in green).
After the surgery, if you want to continue to ventilate the patient, the bronchial blocker is pulled out, leaving behind the standard endotracheal tube to ventilate both lungs.
There are various advantages and disadvantages of double-lumen tubes and bronchial blockers.
Both lumens of a double-lumen tube are wide so you can individually suction both lungs. On the other hand, the lumen of bronchial blockers is generally too small for effective suction, so secretion removal from the blocked lung can be difficult. Double-lumen tubes are bulky and are therefore difficult to insert in a difficult airway. On the other hand, bronchial blockers need only a standard-size endotracheal tube so are easier to insert in this situation. Due to their size, double-lumen tubes are also more traumatic and are usually not used postoperatively for continued ventilation. Bronchial blockers need only standard endotracheal tubes which are much less traumatic and can be easily kept in for postoperative ventilation.
Microlaryngeal Tubes
In anaesthesia, we often talk about sharing the airway with the surgeon. This is especially true for operations involved with the laryngeal inlet. Imagine that the diagram below shows the laryngeal inlet, with the vocal cords shown in red (these diagrams are not drawn to scale). There is a growth on one of the vocal cords (yellow) and the surgeon wants to remove it.
You happily pass a standard endotracheal tube. However, the surgeon isn’t happy because the endotracheal tube is blocking his access to the growth.
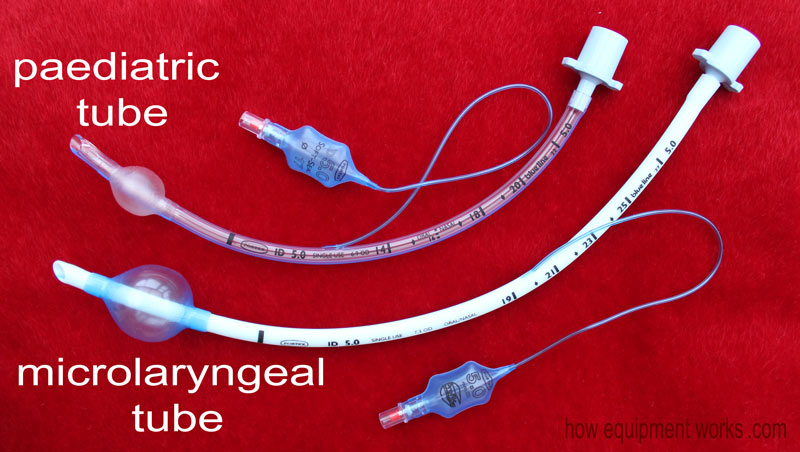
Fortunately for this situation, there is a specially designed tube called a microlaryngeal tube. This tube has a small diameter (e.g. internal diameter of 5 mm) and this is small enough to provide good surgical access to the growth.
Now you might wonder if it is possible to use a paediatric tube with a narrow diameter (e.g. internal diameter of 5 mm) for this purpose. This is not advisable as paediatric tubes are not designed for use in adults. For example, in an adult patient, the pediatric tube may not be long enough.
Also, a paediatric tube used in an adult patient may not have a large enough cuff to provide a good seal.
The micro laryngeal tube is specially designed to avoid these problems. Below are two 5 mm internal diameter tubes, the upper one a paediatric tube and the one below it a microlaryngeal tube. Note that, compared with the paediatric tube, the microlaryngeal tube is longer and has a larger cuff.
This brings my explanation of endotracheal tubes to an end. Hopefully, you now have a good basic overview of this topic. Of course, when using endotracheal tubes clinically, you must be first formally trained in their safe use. Bye.

We have now reached the end of our discussion on tracheal tubes. I hope it has given you a good introduction to the subject and will help you when you read further on this topic. This website is funded mainly by donations, so if you can help, please consider contributing something small as described below. Also, I don’t have an advertising budget, so please do tell your colleagues near and far about this website! Many thanks.

Hello! My name is Pras, and I am the author of this website. I have made the website completely free to access so that people from all over the world can benefit from it.
If you can afford it, I would be very grateful if you would consider making a single donation of one dollar (or the equivalent in your currency) to help cover the expenses needed to run this website (e.g. for special software and computers). For this website to survive, donations are desperately needed. Sadly, without donations, this website may have to be closed down.
Unfortunately, perhaps because many people think that someone else will donate, this website gets only very few donations. If you are able to, please consider making a single donation equivalent to one dollar. With support from people like you, I am sure this educational website will continue to survive and grow. Thank you very much for your support.

