Note: This is part 4 of the discussion of amazing experimental laryngeal mask airways. If you have not read part 1, please click here to go to part 1.
The other Brain!
Dr. Archie Brain is a multitalented person. Apart from all the creativity associated with the laryngeal mask, he also composes music, makes his own guitars (see below !) and plays them as well. He likes to paint, and make sculptures and the occasional piece of furniture. He also likes to ponder about issues in theoretical physics such as the nature of time. He is fluent in many languages (six ?) and is now learning his seventh: Mandarin (Chinese).
I believe it is the fusion of Dr. Archie Brain’s love of science and creativity that gave birth to the laryngeal mask. Now let us get back to the experimental laryngeal masks.
Gastric channel
The upper airway is shared by the respiratory system and gastrointestinal system, which are generally enemies of each other. It is undesirable for gastric contents to go into the lungs and it isn’t good for air to go into the stomach. Normally the epiglottis and esophageal sphincters keep the peace.

Dr. Archie Brain actually thought of this issue very early in the development of the laryngeal mask. Shown below is Dr. Brain’s first mention of the laryngeal mask concept in his notebooks. You can see that regurgitation was something he was thinking even at the very first moments.
A solution explored was to provide a separate pathway for regurgitated fluid to escape to the surface.
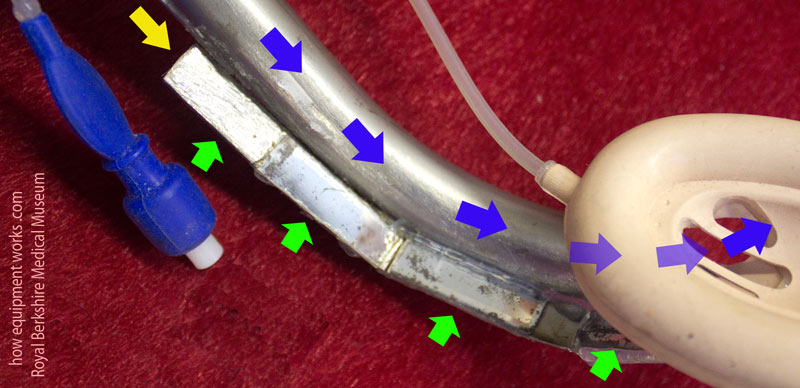
Shown below is an early example of such a channel. The green arrows show the respiratory tube and the blue arrows show the gastric channel. The tip of the gastric channel would protrude into the oesophagus. Dr. Brain considered this too traumatic to use on actual patients.

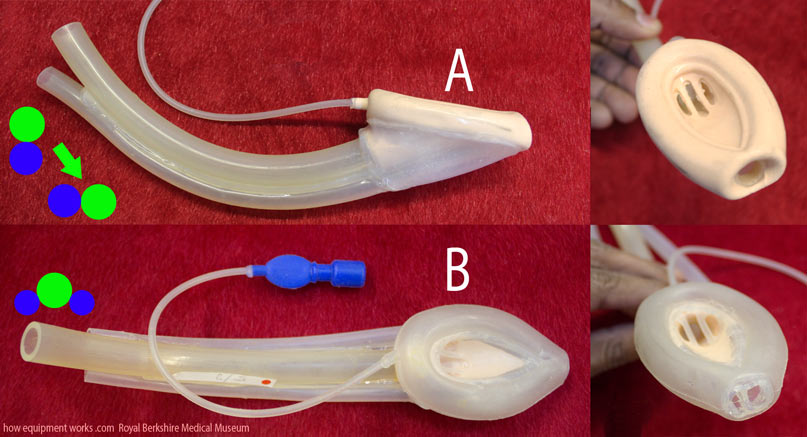
You can see in the experimental laryngeal masks below, that the esophageal opening is much more gentle than the above design. Also note that in example A in the image below, the airway tube is right above the gastric channel. This makes the mask “tall vertically”. To make it easy to insert, the mask was first turned onto a side (green arrow) and once inside, it was rotated back up. Though this mask provided very high-quality seals, Dr. Brain abandoned it because he felt that the vertical tube arrangement was less comfortable for the patient. Example B shows a different design in which there are two gastric channels, one on either side of the airway tube. This made it easier to insert and was much more stable.
Below are some more experimental laryngeal masks where Dr. Brain investigated various oesophageal openings. In the one below, he explored how big he could make the opening.
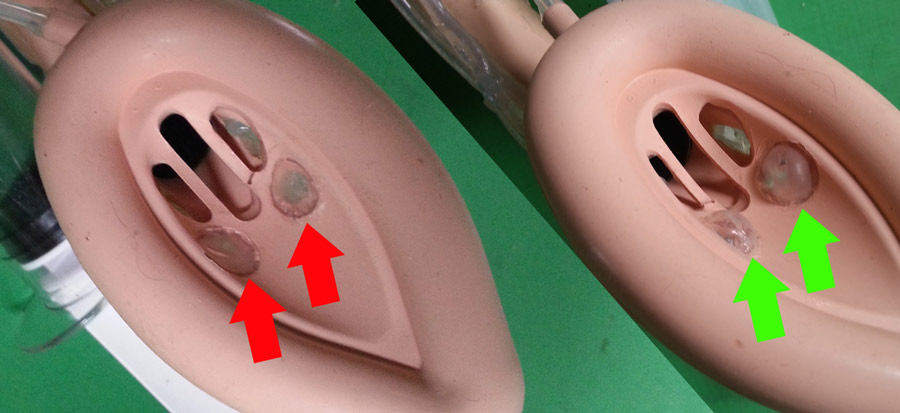
Dr. Brain tried many experimental laryngeal mask designs to try and minimise interfering with the upper oesophagal sphincter. Normally, the oesophagal sphincter is closed (green arrows), preventing material from regurgitating into the pharynx. The insertion of a laryngeal mask can force open this sphincter ( red arrows) and encourage regurgitation.
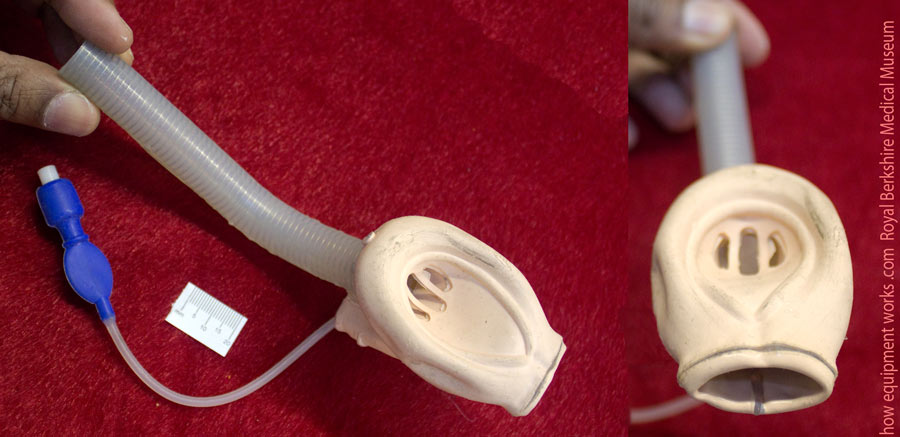
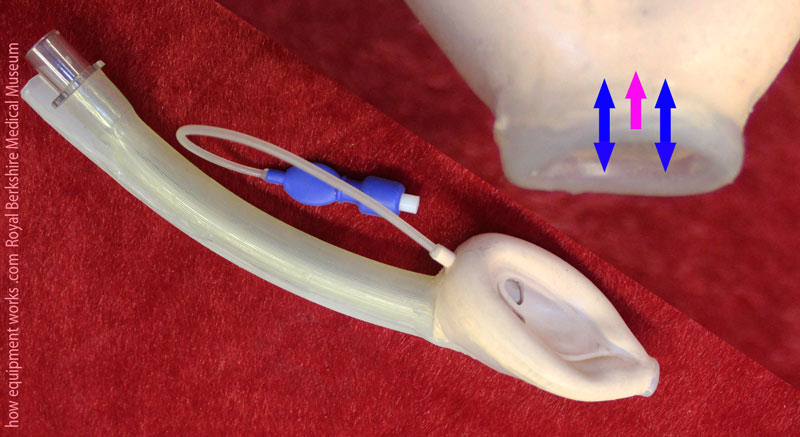
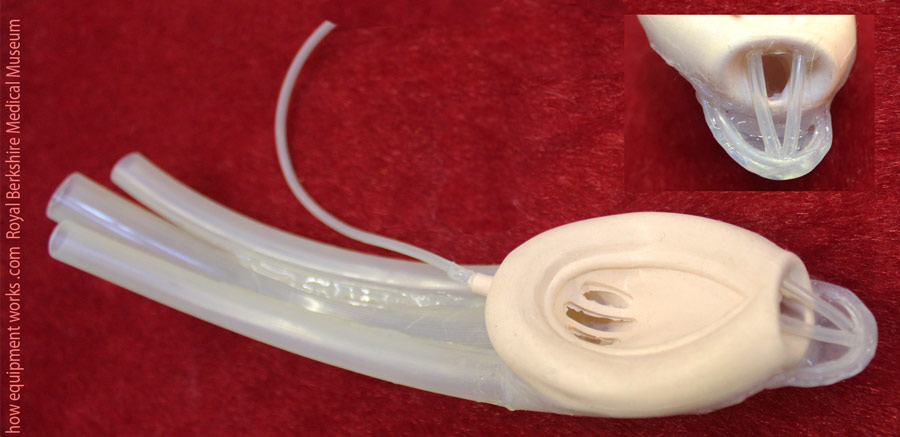
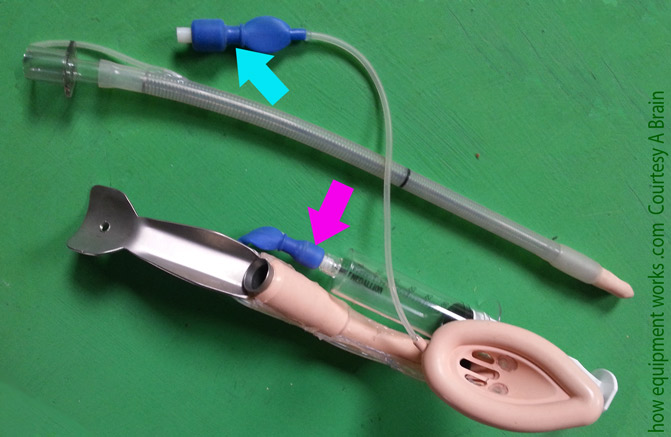
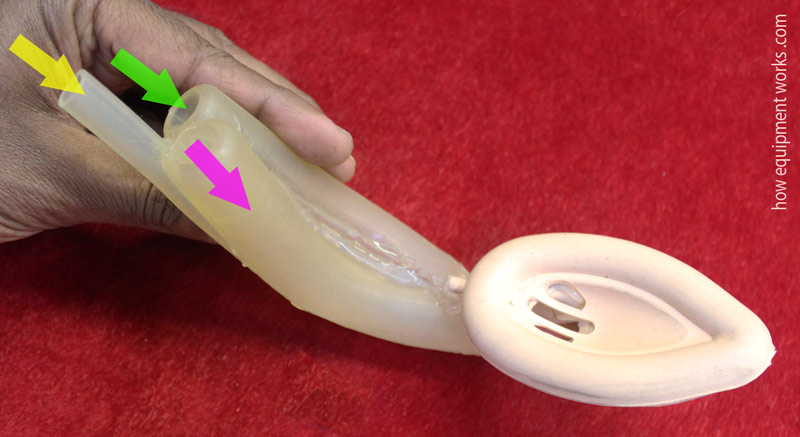
The experimental laryngeal mask shown below had a gastric channel with a specially designed oesophageal opening, shown magnified on your right. The opening was such that it was very flexible ( blue arrows) and also had a slight outward force (pink arrow).
Under normal conditions, the opening of the gastric channel would be compressed by the oesophagal sphincter, and it would remain closed, as shown in the left image below. However, if the oesophagal sphincter opened because the patient was regurgitating, the gastric channel opening would also open at the same time, allowing the material to go through.
The experimental laryngeal mask shown below aimed to maintain the normal shape of the tip of the laryngeal mask to make it easy to insert. Once inserted, gastric fluids could go through the holes into the gastric channel. However, once constructed, Dr. Brain felt that the rubber was too stiff and was likely to cause airway trauma. Therefore it was not used on patients.

Here is another design. In this case, the gastric channel opening has a “lip” extending forward.
A gastric channel, as shown on the left, can make the front of the laryngeal mask rather “blunt”, potentially making it difficult to insert.
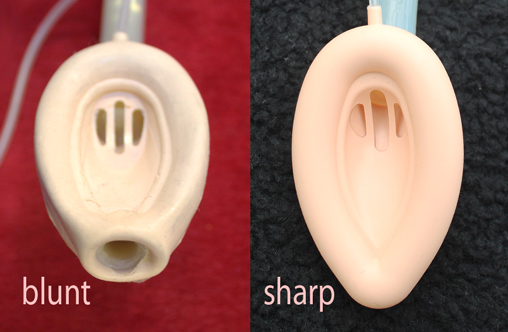
The protruding “lip” in the experimental mask shown before allows the gastric channel to be “sharp” and streamlined.

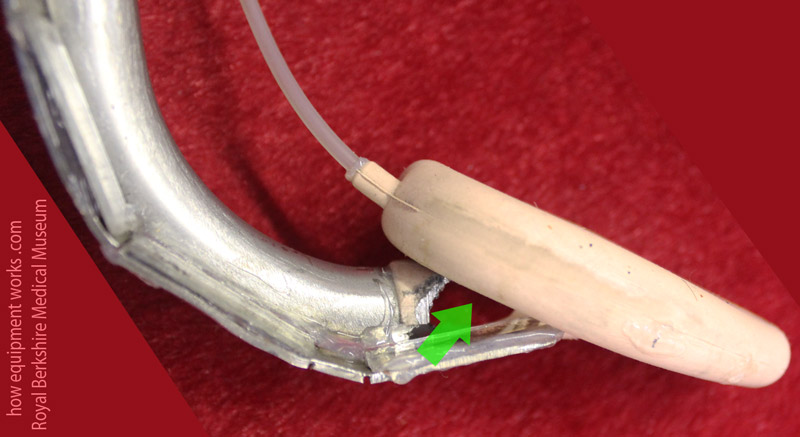
The “lip”, which is shown in green below, with its streamlined shape, guides the laryngeal mask as it is inserted. This is one of many examples where Dr. Brain was trying to make a design that tried to meet many desirable properties: in this case, having a large oesophagal opening while at the same time being easy to insert.
A more radical design that Dr. Brain thought of involved a laryngeal mask with a gastric channel that ended in a cuffed tube that entered the oesophagus.

In this design, when the gastric channel cuff is inflated, it forms a tight seal with the oesophagus.
Dr. Brain abandoned this idea because he felt that if the patient vomited, the tight seal may prevent a quick enough exit of the gastric material, resulting in high esophageal pressures. Such high pressures could then cause tears or even rupture of the oesophagus.

Do you work in the anaesthetic team? If you do, please visit the free website below, which has anaesthesia-related fun and safety material. Click the button below to visit.

Dr. Brain also tried a very different approach. Instead of trying to divert gastric material out through a tube, he explored the concept of letting the material pass under the laryngeal mask and collect in the pharynx.
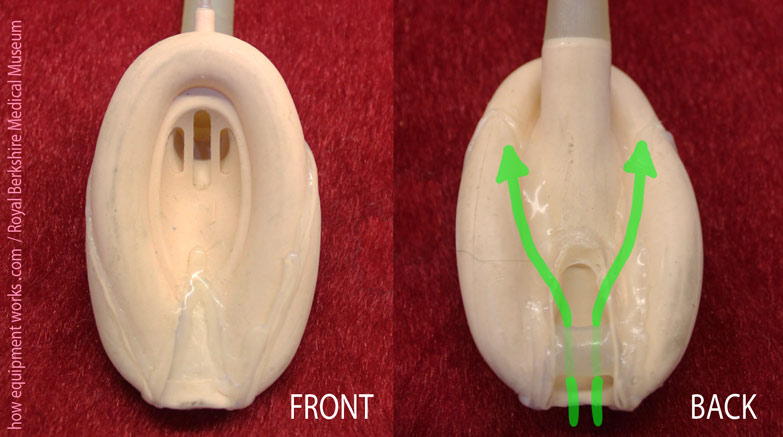
Here is an early experimental laryngeal mask showing this concept. The rear of the mask has a groove through which regurgitating gastric material can pass (green arrows).

Here is another design using the same concept. The green arrows show the path regurgitant gastric contents would take.
Intubation aid
It is often thought that tracheal tubes and laryngeal masks are not the “best of friends”. After all, thanks to the laryngeal mask, the need to intubate has declined markedly.
However, the reality is very different. While the number of tracheal intubations has declined, there are still clinical indications where it is very necessary to intubate a patient. Far from being enemies, the laryngeal mask, in certain situations, actually helps the tracheal tube achieve its task.
Early in the development of the laryngeal mask, Dr. Brain appreciated that the laryngeal mask directly faced the tracheal inlet. This led to the idea that a tracheal tube which is passed inside a laryngeal mask tube was likely to naturally go into the trachea.
Here is an early experimental laryngeal mask designed to allow intubation. The green bar (pink arrow) is there to prevent the epiglottis from falling in and causing blockage. This bar was attached diagonally to allow a tracheal tube (represented by the blue arrow) to pass by its side.

I will now be showing you some very unique experimental intubating laryngeal masks. Look at the intubating laryngeal mask below. It has two places to inflate it (arrows). One is to inflate the main cuff (blue arrow). Can you guess what the other inflation port (pink arrow) is for?
If you look closely, you will see two mysterious “eyes” (red arrows)! These two “eyes” are actually tiny little balloons. Using a separate inflation tube to the one used for the main cuff (the pink arrow in the image above), you can inflate and deflate these tiny balloons. Can you guess what these balloons were for?
The mystery balloons are represented by the pink balloon in the image below. In diagram ( A ), while intubating through the laryngeal mask, the tracheal tube hits the posterior boundary of the laryngeal inlet and therefore not go into the trachea. In this situation, the balloons can be inflated. As shown in diagram ( B ), the inflated balloons lift the tracheal tube so that it can now pass into the trachea.
The next experimental intubating laryngeal mask has three tubes! The yellow arrow points to the gastric channel leading to an esophageal opening not visible in this image. The green arrow shows the lumen to which you fix the breathing system. While the patient is safely breathing, you can take your time and intubate using the lumen shown by the pink arrow!
Look at this experimental intubation laryngeal mask. Can you guess how this works?

In this design, you pass the tracheal tube through the tube shown with blue arrows in the image below. Now here is the magic. On the side of the breathing tube are small mirrors (green arrows). When you try to intubate, you will see ( yellow arrow) on the mirrors a reflection of the tube passing into the trachea.
Here is another view of this interesting concept. The green arrow shows a “window” through which you would, via the mirrors, see the tracheal tube pass into the trachea. This experimental version was considered too traumatic to use on actual patients. It is important to remember that at the time of this concept, modern low-cost miniature camera technology like that found in devices such as video laryngoscopes was not available. Dr. Brain was trying his best to improvise using the materials available at that time.
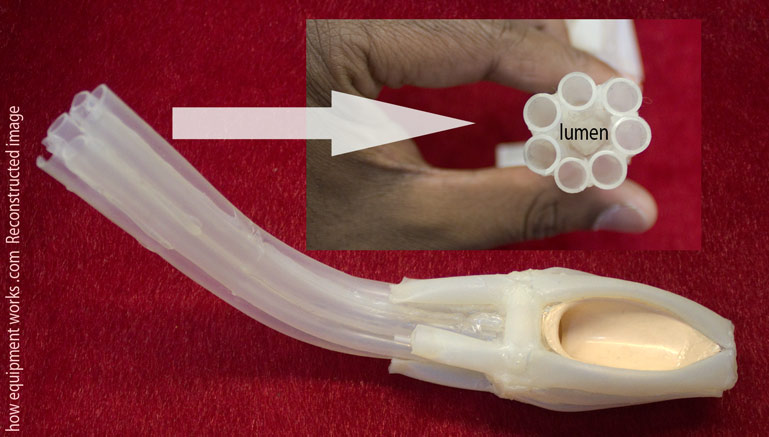
The most exotic design!
To me, the next experimental laryngeal mask is the most “beautiful” one. When I first saw it, I just couldn’t make out how it worked. It looked like a creature from the deep sea. It is actually a very “soft” gentle device. The patient gases go through the area labelled as “lumen” in the diagram. There are seven tubes, which are very soft to the touch, that surround the lumen. These seven tubes don’t conduct any gases. Instead, they are there to form a soft padded wall around the lumen which is kink-resistant. Dr. Brain made this to see how it would look. It was not used in patients.
The story is not over!
As you have seen, the laryngeal mask was not something invented overnight. Dr Archie Brain spent many years with his mind and hands to bring to reality this marvellous airway device that has transformed the practice of anaesthesia. So many millions of patients have benefited from his invention. When you next use a laryngeal mask or similar device, have a good look at it. Many of the features you see now in modern devices originated decades ago in the experimental laryngeal masks made by Dr. Brain.

I have now come to the end of this section. I hope you have enjoyed this journey as much as I have. However, the story of the laryngeal mask is not over. Like everything else in the world of science, the laryngeal mask and similar devices can be improved further. I hope this web page has inspired you to think of designing the next version!

Hello! My name is Pras, and I am the author of this website. I have made the website completely free to access so that people from all over the world can benefit from it.
If you can afford it, I would be very grateful if you would consider making a single donation of one dollar (or the equivalent in your currency) to help cover the expenses needed to run this website (e.g. for special software and computers). For this website to survive, donations are desperately needed. Sadly, without donations, this website may have to be closed down.
Unfortunately, perhaps because many people think that someone else will donate, this website gets only very few donations. If you are able to, please consider making a single donation equivalent to one dollar. With support from people like you, I am sure this educational website will continue to survive and grow. Thank you very much for your support.

